Are airborne droplets driving new cases of COVID-19? Why are airborne droplets not yet officially recognized, or at least considered, as a mode of transmission?
Update: 7/13/2020. This article was written and readied for publishing just days before the latest WHO guidance published July 9th, 2020. The quotes sourced before the WHO’s updates will remain unchanged as a reflection of historical precedence.
8/11/2020: A research team at the University of Florida succeeded in isolating live virus from aerosols collected at a distance of seven to 16 feet from patients hospitalized with Covid-19 — farther than the six feet recommended in social distancing guidelines. – NYT
9/21/2020: CDC removes references to airborne transmission of COVID-19 from website content. – NYT
Specifically, scientists in 32 countries worry: “The risk of airborne transmission has not been recognized by the WHO [World Health Organization], except in some health care settings.” Further, scientists have called into question the role of indoor air quality.
Should one assume that COVID-19 spreads only by large droplets — or — does the evidence support the aerosolized spread of COVID-19?
The WHO cites findings from laboratory-based experiments that do not “reflect clinical conditions”. However, WHO has produced limited counter-factual evidence. Reasonably, the WHO has also pointed out that many new and recent studies have yet to receive peer reviews.
Below you’ll find a body of facts, studies, and WHO statements exploring both sides of the issue.
Airborne Droplets – Nuclei Aerosols Explained – Mechanisms and Characteristics
Before addressing the data, science, and commentary of the discussion herein, consider how the size of a particle or droplet influences the character of an infectious bio-aerosol.
Virus-laden particles vary in complexity and characterization. The composition may include various components including salts, proteins, and other organic and inorganic matter, including virus particles.
Airborne Particle Size
The size of an infectious particle has multiple implications, both in its ability to transfer through the air and penetrate natural or artificial antimicrobial defenses.
Aerosol physics explains how particle size and composition affect bouncy, deposition, drift area, suspension time, and viral payload.
Particle Characteristics
The deposition pattern can be influenced by several factors: (1) particle characteristics, such as particle size, shape, density, charge, and hygroscopicity; (2) airway geometry as a function of gender, age, and diseases status; and (3) breathing pattern, including frequency, tidal volume, and breath-holding time.
Mechanisms of Pharmaceutical Aerosol Deposition in the Respiratory Tract
Infectious particles released into the air are most often compared by demonstrating the differences between an uncovered sneeze versus a masked cough. However, there are other mechanisms of aerosol production including running water from sinks and toilets, medical procedures, medical devices, breathing, and talking. Individual factors also influence the quantity and size of droplet emissions such as the host’s body structure and airway geometry.
Particle Size and Inhalation
The ability of the particle to enter the head airway, also known as its inhalability, is a function of its aerodynamic diameter. Inhalability is a fraction of airborne particles entering the human airway. Most of the experimental data on inhalability has been obtained in aerosol wind tunnels. Inhalability has been found to be near 100% for particles smaller than 5 μm, based on these wind tunnel studies (24). The inhalability decreases as the particle size increases and stays at 50% for particles greater than about 50 μm (24,25).
Mechanisms of Pharmaceutical Aerosol Deposition in the Respiratory Tract
Particles larger than 10 um are most easily intercepted by the upper airways. Larger particles tend to fall to the floor or surfaces, while smaller particles become buoyant and remain airborne for longer periods of time.
Droplets, by definition, are considered as liquid particles larger than 5 um.
Particles smaller than 5 um, widely categorized as aerosols, are able float longer in the air and penetrate far deeper into the lungs.
What are the Differences Between Droplets vs Aerosols (Droplet Nuclei)
Droplet Size Definitions
“Respiratory infections can be transmitted through droplets of different sizes: when the droplet particles are >5-10 μm in diameter they are referred to as respiratory droplets, and when then are <5μm in diameter, they are referred to as droplet nuclei.1 According to current evidence, COVID-19 virus is primarily transmitted between people through respiratory droplets and contact routes.2-7″
Below we’ve aggregated studies which make the case for and against each perspective.
Airborne Transmission vs Droplet Transmission
Airborne transmission is different from droplet transmission as it refers to the presence of microbes within droplet nuclei, which are generally considered to be particles <5μm in diameter, can remain in the air for long periods of time and be transmitted to others over distances greater than 1 m.
World Health Organization – Modes of transmission of virus causing COVID-19
Rethinking Airborne Spread of COVID-19
Ideologically, deciding whether an agent is airborne impacts the types (and costs) of infection control interventions.
Over 200 scientists agreed that risk factors associated with smaller viral laden particles (aerosols or viral nuclei) have been underrepresented in popular guidance issued by WHO.
July 6th, 2020 scientists wrote an open letter to the World Health Organization (WHO) titled, “It is Time to Address Airborne Transmission of COVID-19“. The letter is published in the journal Clinical Infectious Diseases.
Scientists: Potential for Airborne Spread of COVID-19
“We appeal to the medical community and to the relevant national and international bodies to recognize the potential for airborne spread of COVID-19. There is significant potential for inhalation exposure to viruses in microscopic respiratory droplets (microdroplets) at short to medium distances (up to several meters, or room scale), and we are advocating for the use of preventive measures to mitigate this route of airborne transmission.”
The paper goes on to state, “droplets smaller than (<0.5 micron) remain airborne and pose a risk of exposure at distances beyond 1 to 2 m”.
Social Distancing & Aerosols
“Unfortunately, these measures [social distancing] do not prevent infection by inhalation of small droplets exhaled by an infected person that can travel a distance of meters or tens of meters in the air and carry their viral content.”
The authors believe that airborne transmission is possible and that HVAC systems when “not adequately used may contribute to the transmission of the virus, as suggested by descriptions from Japan, Germany, and the Diamond Princess Cruise Ship.”
World Health Organization (WHO) Stance on Reporting of Airborne COVID-19 Transmission
Scientific debate is not new to most following the continued guidance from the World Health Organization (WHO) since declaring SARS-COVID-2 a global pandemic.
As of June 7th, 2020: the WHO website states: “The Scientific brief on Modes of transmission of the virus causing COVID-19: implications for IPC precaution recommendations is currently being updated.” On page information was updated June 9th.
The WHO’s stance on droplet versus airborne transmission is not well supported by counter-factual data. WHO maintains that aerosol COVID-19 transmissions have only been reported during medical invasive procedures of COVID-19 patients.
Study in Question: Droplets and Aerosols in the Transmission of SARS-CoV-2
The WHO has previously reported, “In an analysis of 75,465 COVID-19 cases in China, airborne transmission was not reported.“
The WHO acknowledges previous findings from laboratory-based experiments, referencing this study published in the New England Journal of Medicine about aerosolized viral spread, concluding data does not “reflect clinical conditions”.
WHO: Experimental Studies Don’t Reflect Human Cough Conditions
“In this experimental study, aerosols were generated using a three-jet Collison nebulizer and fed into a Goldberg drum under controlled laboratory conditions. This is a high-powered machine that does not reflect normal human cough conditions. Further, the finding of COVID-19 virus in aerosol particles up to 3 hours does not reflect a clinical setting in which aerosol-generating procedures are performed—that is, this was an experimentally induced aerosol-generating procedure”
Scientists at WHO note pitfalls in studies conducted within controlled environments versus real-world clinical settings. In live scenarios, room air is heavily laden with extraneous particles, both those shed from humans and those produced in the environment.
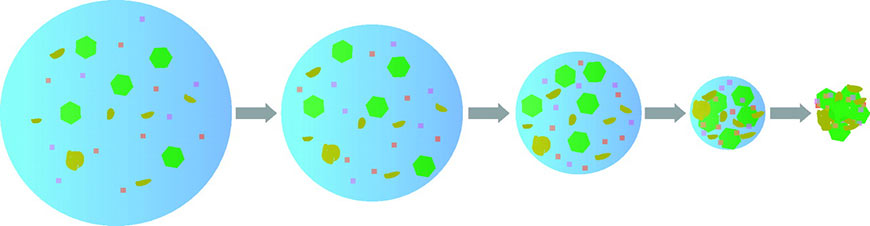
Study: Final Droplet Size Depends on Relative Humidity
“Artificially produced aerosols are normally used in controlled environments where there are no other aerosols to which the nebulized particles can bind. They are thus influenced only by the size of the original droplet created by the nebulizer and by the solute concentration in the droplet. When a droplet evaporates (Fig. 2), its final size (the droplet nucleus) depends on the relative humidity (RH) in the chamber. To some extent, this phenomenon can also be observed with natural aerosols.”
Study: American Society for Microbiology – Methods for Sampling of Airborne Viruses
Particles in the air tend to clump together, while also being subject to natural and artificial air currents. These conditions and variables are difficult to recreate in artificial environments.
Read More: Particulate Size & Characterization
Particle Behavior Under Dynamic Conditions
Airborne viral particles are directly observable but technological limitations prevent researchers from discerning non-viable (dead / non-functional) virus fragments from the actual live virus. Not all live viruses are able to replicate a physiological niche for their own reproduction. Finally, the minimal infectious dose is still unknown, thus the aerosol transmission distance cannot be strictly determined.
“Microbiologists, like characters in zombie fiction, quickly learn the critical importance of distinguishing the living from the dead.”
Dead or Alive: Molecular Assessment of Microbial Viability
WHO questions studies based on PCR-based assays are not indicative of a viable virus RNA in air samples.
“WHO is aware of other studies which have evaluated the presence of COVID-19 RNA in air samples, but which are not yet published in peer-reviewed journals. It is important to note that the detection of RNA in environmental samples based on PCR-based assays is not indicative of viable virus that could be transmissible.”
(World Health Organization)
Air Sampling Tests of Airborne Droplets vs Real-World Conditions
Clinical settings don’t reflect environments and behaviors found in general populations. Scientists express concerns over waiting for a “silver bullet” as direct evidence of aerosol transmission.
Aerosols perform differently in clinical controlled environments — that’s partly because social interactions are limited and environmental settings are diligently constructed. Temporary triage rooms allow pop-up construction of negative pressure isolation areas. Isolation areas, negative pressure rooms, HEPA filtration, air change rates, and clean/dirty corridors, including thermohygrometric design, are reasons why non-procedural bio-aerosol exposure in healthcare environments is less unlikely.
From floor to ceiling, even moderate and practical HVAC can create log reductions in airborne contamination.
A comparison of apples and oranges occurs when two items or groups of items are compared that cannot be practically compared.
The exact mechanism of the novel Sars-COVID-2 virus is widely unknown, however it is becoming better understood. Widely known, is that droplet-based viruses proliferate among larger, dense clusters of people where direct contact, direct communication, shared objects, and close proximity are sustained over extended periods.

Contrasting Differences in Environmental Controls
How does indoor air quality, ventilation, and air conditioning affect the spread of airborne contamination?
In the most critical environments, primary and secondary engineering controls are structural mechanisms in anticipation of product contamination, hazardous substances, and infectious diseases.
Engineering controls might include local exhaust ventilation, structural partitions, negative pressure differentials, and isolation areas.
Hospital air quality is not extraordinarily clean in comparison to high-performance cleanroom systems. Wards housing COVID patients, or any infectious disease, are quarantined to areas with engineering controls such as overall negative pressure, isolation areas, physical barriers, and controlled access.
- Negative Pressure Hospital Rooms
- Hardwall Triage Structures and Ceilings
- Air Change Requirements for Hospital Containment Zones
- Softwall Curtain Containment with Negative Airflow Exhaust
Should Ventilation and Air Quality Be Prioritized in the Prevention of COVID Transmission?
“In general, very low or undetectable concentrations of airborne SARS-CoV-2 were found in most of the patient areas of Renmin Hospital, suggesting that the negatively pressurized isolation and high air exchange rate inside the intensive care units, coronary care units and ward room of Renmin Hospital are very effective in limiting the airborne transmission of SARS-CoV-2. The highest concentration in patient areas was observed inside a patient mobile toilet room at Fangcang Hospital (19 copies m−3), which is a temporary single toilet room of approximately 1 m2 in area without ventilation.”
Relative humidity is a factor in the maximum infectivity of airborne viruses. For example, influenza viruses are most infectious in low RH conditions, while Rhinovirus and Poliovirus are most infections in high humidity environments.
Related: Characterizing Problematic Air Behavior in HVAC Systems
Studies Supporting Airborne Transmission of COVID-19
New studies point to airborne spread as a driver of COVID-19 infections.
Study: Airborne Transmission Virulent and Dominant for COVID-19 Spread
A study published June, 30th 2020 states:
“Our results show that the airborne transmission route is highly virulent and dominant for the spread of COVID-19. The mitigation measures are discernible from the trends of the pandemic. Our analysis reveals that the difference with and without mandated face covering represents the determinant in shaping the trends of the pandemic. This protective measure significantly reduces the number of infections.”
Study: Identifying airborne transmission as the dominant route for the spread of COVID-19
Authors reference studies that show that environments are capable of hoisting and retaining infectious particles in the air. Specifically, buoyant particles from human coughs.
Study: We propose that SARS-CoV-2 may have the potential to be transmitted through aerosols.
“Such viral particles are known to be encapsulated in globs of mucus, saliva, and water, and the fate/behavior of globs in the environment depends on the size of the globs. Bigger globs fall faster than they evaporate so that they splash down nearby in the form of droplets (Grayson et al., 2016; Liu et al., 2016). Smaller globs evaporate faster in the form of aerosols, and linger in the air, and drift farther away than the droplets do.”
Study: High Concentrations of Viral RN with Aerosol Size Distributions
“We found that some medical staff areas initially had high concentrations of viral RNA with aerosol size distributions that showed peaks in the submicrometre and/or supermicrometre regions; however, these levels were reduced to undetectable levels after implementation of rigorous sanitation procedures. Although we have not established the infectivity of the virus detected in these hospital areas, we propose that SARS-CoV-2 may have the potential to be transmitted through aerosols.“
Study: Aerodynamic analysis of SARS-CoV-2 in two Wuhan hospitals
Study: Aerodynamic Diameter of 20 μm or 10 μm or Less Should be Recognized as Aerosols
“Conversely, there have been some other postulations, indicating that aerodynamic diameter of 20 μm or 10 μm or less should be reckoned to be aerosols, based on their ability to linger in the air for a prolonged period, and the reachability to the respirable fraction of the lung (alveolar region) (Gralton et al., 2011; Nicas et al., 2005; Tellier, 2009). Small aerosols are more susceptible to be inhaled deep into the lung, which causes infection in the alveolar tissues of the lower respiratory tract, while large droplets are trapped in the upper airways (Thomas, 2013).”
Samples of Air Outlet Exhausts Indicate Airborne COVID Transmission
Ong et al. (2020) have studied the sources of COVID-19 that could transmit the infection during the involvement in healthcare services. The results obtained from their study indicate that the samples collected from the personal protective equipment (PPE) worn by the hospital staff (physicians exiting the patient rooms) were negative for COVID-19. However, the samples from the air outlet exhaust fans in patient-rooms except corridors and anterooms have been reported as positive for COVID-19, indicating that the airborne transmission is plausible
However, some droplets, when ejected from an infected person, convert to aerosol particles (also known as bioaerosols) with relatively smaller aerodynamic diameters and, consequently, become airborne (Morawska, 2006). Such virus-laden aerosol particles are capable of infecting people who inhale such particles, thereby spreading the disease.
Study: Results Indicate SARS-CoV-2 Aerosol & Nosocomial Spread Plausible
Our results indicate that aerosol and fomite transmission of SARS-CoV-2 is plausible, since the virus can remain viable and infectious in aerosols for hours and on surfaces up to days (depending on the inoculum shed). These findings echo those with SARS-CoV-1, in which these forms of transmission were associated with nosocomial spread and super-spreading events,5 and they provide information for pandemic mitigation efforts.
Study: Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1
Study: Are Aerosol Particles Spread by Air Currents?
Breathing and talking also produce smaller and much more numerous particles, known as aerosol particles, than those visualized in the laser experiment of Anfinrud and colleagues.2-4 Certain persons called “super spreaders” produce many more aerosol particles than other persons. The diameters of these particles are in the micron range. These particles are too small to settle because of gravity, but they are carried by air currents and dispersed by diffusion and air turbulence.
Study: Droplets and Aerosols in the Transmission of SARS-CoV-2
Paper: COVID-19 Airborne Transmission: The World Should Face the Reality
Similar papers have also been published calling for revised considerations and wider bodies of evidence. On April 10th, 2020 a paper was published in PubMed:
“The air transmission issue should be taken seriously now, during the course of the epidemic.”
The authors voice concerns over failure to take airborne spread “seriously”. Empirical data may never provide a silver bullet. Studying aerosol transmission of infectious diseases is challenging, as it is very difficult to recreate real-world conditions in laboratory scenarios.
“If this [airborne spread] is the case, it will take at least several months for this to be confirmed by science. This is valuable time lost that could be used to properly control the epidemic by the measures outlined above and prevent more infections and loss of life….”The air transmission issue should be taken seriously now, during the course of the epidemic.” –
Paper: Airborne transmission of SARS-CoV-2: The world should face the reality“.
Droplet vs Airborne Precautions: Wear a Mask
A preponderance of the evidence suggests that while proof for aerosol transmission of COVID-19 may not be empirically clear, it was convincing enough for 239 scientists to call upon the WHO to recognize, revisit, and reconsider the possibility of airborne SARS-Cov-2 transmission.
Study: Social Distancing Far From Established Scientific Evidence
Though social distancing would be promising in combating the COVID-19, the minimum distances that have been maintained between an infected person and a host are disputable and far from being established based on any scientific evidence.
“One could dispute that, unlike larger droplets, aerosols may pose a greater risk of the spread of the COVID-19 disease among many susceptible hosts positioned far from the point of origin.”
In a previous post, we covered various examples of crossed wires and mixed messaging among tried and true methods of contamination control.
The WHO has also noted how the internet and modern communication fuel both patterns of improved health outcomes, and also patterns of misinformation, rumors, and conspiracy theories.
“Numerous examples show that these platforms can improve health outcomes.1 Unfortunately, the same powerful tools can be used to share health related misinformation, disinformation, rumors and conspiracy theories. Misinformation hampers public health responses to epidemics and can result in people taking fewer measures to prevent disease transmission effectively.2 The dynamics of the spread of misinformation are complex, probably multi-faceted and poorly understood. Patterns of misinformation spread and the characteristics of networks at the macro level indicate that both individuals and communities are vulnerable to misinformation.”
WHO – Infodemic management: a key component of the COVID-19 global response
Study: Direct Evidence is Limited
“When we apply the principles of evidence-based medicine to public policy, there is high-quality, consistent evidence that many (but not all) cloth masks reduce droplet and aerosol transmission and may be effective in reducing contamination of the environment by any virus, including SARS-CoV-2. No direct evidence indicates that public mask wearing protects either the wearer or others.”
Study: Cloth Masks May Prevent Transmission of COVID-19: An Evidence-Based, Risk-Based Approach
Face masks and face coverings are virtually the only widely available universal source control measure for non-contact interactions and will reduce the number of airborne virus droplets.
Updated Guidance – Does WHO Acknowledge Airborne Transmission of COVID-19?
WHO Considers Role of Indoor Aerosol Spread, Particularly when Ventilation is Poor
“Airborne transmission of SARS-CoV-2 can occur during medical procedures that generate aerosols (“aerosol-generating procedures”).(12) WHO, together with the scientific community, has been actively discussing and evaluating whether SARS-CoV-2 may also spread through aerosols in the absence of aerosol-generating procedures, particularly in indoor settings with poor ventilation.”
WHO States Aerosol Transmission “Has Not Been Demonstrated”
“To date, transmission of SARS-CoV-2 by this type of aerosol route has not been demonstrated; much more research is needed given the possible implications of such route of transmission.”
“Recent clinical reports of health workers exposed to COVID-19 index cases, not in the presence of aerosol-generating procedures, found no nosocomial transmission when contact and droplet precautions were appropriately used, including the wearing of medical masks as a component of the personal protective equipment (PPE).”
WHO Suggests Aerosol Transmission Cannot Be Ruled Out
“Outside of medical facilities, some outbreak reports related to indoor crowded spaces (40) have suggested the possibility of aerosol transmission, combined with droplet transmission, for example, during choir practice (7), in restaurants (41) or in fitness classes.(42) In these events, short-range aerosol transmission, particularly in specific indoor locations, such as crowded and inadequately ventilated spaces over a prolonged period of time with infected persons cannot be ruled out. However, the detailed investigations of these clusters suggest that droplet and fomite transmission could also explain human-to-human transmission within these clusters.”
WHO Concedes to Widespread Adoption of Face Masks
“Given that infected people without symptoms can transmit the virus, it is also prudent to encourage the use of fabric face masks in public places where there is community transmission[1] and where other prevention measures, such as physical distancing, are not possible.(12) Fabric masks, if made and worn properly, can serve as a barrier to droplets expelled from the wearer into the air and environment.(12) However, masks must be used as part of a comprehensive package of preventive measures, which includes frequent hand hygiene, physical distancing when possible, respiratory etiquette, environmental cleaning and disinfection.”
March 29th 2020: Modes of transmission of virus causing COVID-19: implications for IPC precaution recommendations
July 9th 2020: Transmission of SARS-CoV-2: implications for infection prevention precautions
The Last Word
“…the use of a mask alone is insufficient to provide an adequate level of protection or source control, and other personal and community level measures should also be adopted to suppress transmission of respiratory viruses.”
WHO – June 5, 2020 – Interim Guidance
Sanitation and hand washing alone will not prevent aerosol spread of infectious diseases. Studies herein show that bio-aerosols are detectable among airborne samples of COVID patients. Further study is required to determine which transmission method is most opportunistic.
Facilities, communities, and organizations must temporally consider the plausibility of infectious spread despite social distancing, which previously was regarded as a distance of 2m (6 feet).
An end-to-end contamination control strategy must recognize both droplets and aerosols. For droplets, hand washing stations, social distancing signage, workstation dividers and adequate sanitation products cannot be overstated. For aerosols, face masks and environmental controls are more meaningful especially when considering the systemic benefits of overall bio-burden reductions.
Who Are We?
Production Automation Corporation (that’s us) is an essential business supplier and consultant for medical device, cleanroom, and general manufacturing industries.
Our staff includes a culture of specialists, entrenched manufacturing partnerships, and decades of experience in the distribution and application of critical and industrial cleaning science.
All products featured on the PAC blog are available through the gotopac.com webstore. Online orders are shipped and fulfilled Monday – Friday from PAC warehouses in California, Minnesota, and Texas.
Production Automation Corporation (PAC) stands 100% behind a product catalog of over 30,000 products, which includes support for factory warranties, value-added services, and returns. Get help from a PAC sales rep during business hours via email, phone, or live chat.
We have answered hundreds, if not thousands of questions about the what, where, why, and how of sanitation and cleaning processes. Have questions? We have answers. Either leave a comment below, or email us directly.

How Have Face Masks Changed Over Time? A Brief History of Face Coverings
Masks were not always made from advanced textiles and multilayer construction. What makes these materials so meaningful when manufacturing PPE equipment, and how has mask technology changed over time?

Where Can I Buy FDA Approved KN95 Masks?
When you buy face masks from PAC you’ll have the benefit of masks shipped from USA warehouses, in-stock availability, and bulk pricing.

What’s a Medical Mask? Why is It Different from a Procedural Mask?
Medical masks by definition, must be validated at a minimum of ASTM Level 1.
Droplets vs Airborne – Science of Airborne Droplets, Aerosols, Particles, and Face Masks
Aerosols vs Droplets – does COVID-19 spread by aerosols or droplets? Does evidence support airborne coronavirus? 15+ studies on COVID particle size, droplets, ventilation, and face masks.

Why 3-Ply Face Masks are Meaningful Alternatives to N95 Masks
How effective are surgical masks and procedural masks as alternatives to N95 masks? Where can I find a reliable supplier of face masks?